
In 2020, Cochrane published a meta-analysis on saturated fat with the following conclusion (1):
The review found that cutting down on saturated fat led to a 17% reduction in the risk of cardiovascular disease . . .
As I stated in other posts, this conclusion is unjustified. For example, the review included a possible fraudulent trial (see here) and trials that could not evaluate the effects of saturated fat (see here). If these trials are excluded, the result becomes weak and non-significant.
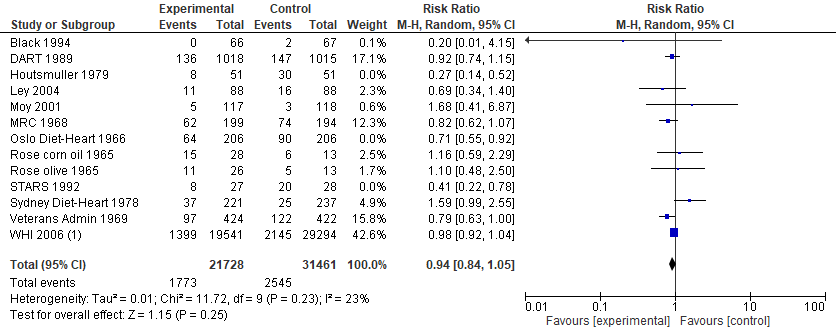 (Image: Cochrane's analysis after exclusion of three trials that should never be included in the first place. Note also that heterogeneity is reduced, from I² = 67% in original analysis to I² = 23% with the three trials excluded)
(Image: Cochrane's analysis after exclusion of three trials that should never be included in the first place. Note also that heterogeneity is reduced, from I² = 67% in original analysis to I² = 23% with the three trials excluded)
There is, however, another aspect of Cochrane's analysis that should be highlighted. If we simply exclude the soft endpoints from Cochrane's analysis (e.g., angina) — leaving a combined endpoint of mostly cardiovascular deaths, non-fatal heart attacks, and non-fatal strokes — the claimed significant reduction in cardiovascular events will again disappear.
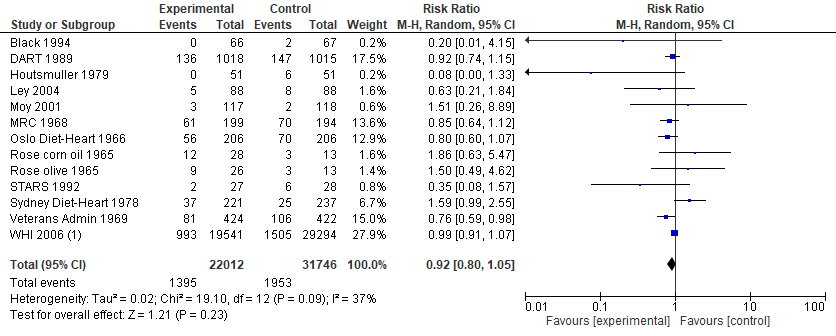 (Image: Cochrane's analysis after excluding the very soft, subjective cardiovascular events. Removing trials at a high risk or unclear risk for "Blinding of outcome assessment" would give a similar result)
(Image: Cochrane's analysis after excluding the very soft, subjective cardiovascular events. Removing trials at a high risk or unclear risk for "Blinding of outcome assessment" would give a similar result)
In other words, the alleged reduction in cardiovascular events was driven by endpoints more susceptible to bias.
Thus, the most important results are those on the harder, more reliable endpoints.
The Endpoint of Total Mortality
In 2012, Cochrane stated the following (2):
Total mortality was examined as it is an important outcome, and there is little likelihood of ascertainment or diagnostic bias which may occur with cause-specific event outcomes.
Indeed, cardiovascular pathologists long noted substantial diagnostic errors for cause-specific events (3). Also, Dayton and Pearce — who conducted a trial in Cochrane's analysis — stated that total mortality was the "most objective and most meaningful of end-points" (4).
More recently in 2021, Jakobsen and colleagues emphasized the importance of considering total mortality (5):
Due to the many methodological limitations, we believe that disease-related mortality should not be used as a primary outcome in many circumstances. Disease- related mortality should primarily be used as a secondary or an exploratory outcome, depending on the envisaged power of the outcome, and results of disease-related mortality should always be related to results of all-cause mortality.
Therefore, one of the most critical questions is: Does a lower saturated fat intake decrease the risk of mortality?
Saturated Fat and Total Mortality
Cochrane's analysis for saturated fat and total mortality consisted of 12 data-sets comprising 3,518 deaths.
What did they find?
As the following image shows, Cochrane found "little or no effect of lower saturated fat compared to higher saturated fat intake on mortality" (1).
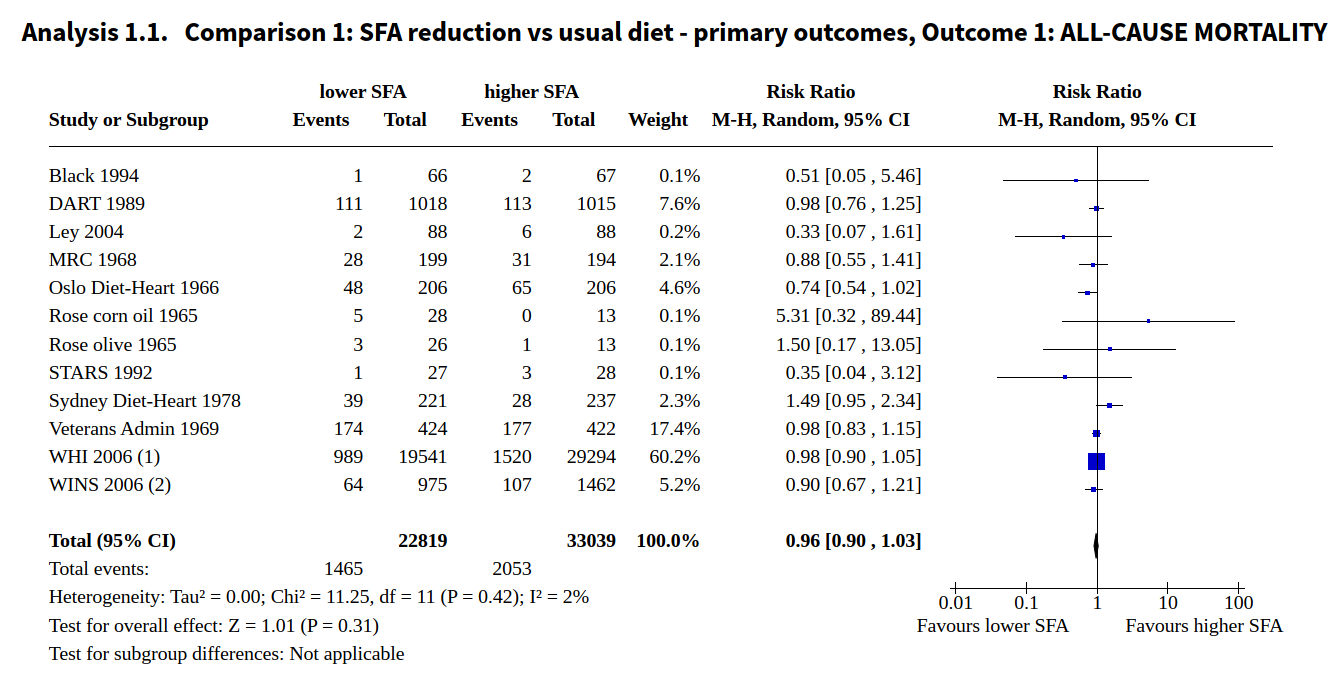 (Image: Taken from Cochrane's published review)
(Image: Taken from Cochrane's published review)
Importantly, this lack of effect held in various sensitivity analyses. To quote (1):
This lack of effect was confirmed in sensitivity analyses including only trials at low summary risk of bias, that aimed to reduce saturated fat, that significantly reduced saturated fat intake, that achieved a reduction in total or LDL cholesterol, excluding the largest trial, or analysing using Mantel-Haenszel or Peto fixed-effect analysis.
And:
There was little or no effect, regardless of what nutrients were used to replace the saturated fat removed, including replacement with PUFA, MUFA, CHO and/or protein. Effects did not differ by main substitution, study duration, baseline saturated fat intake, degree of difference in saturated fat between arms, participant sex, by baseline CVD risk, by degree of cholesterol reduction or by decade of publication.
Excluding trials confounded by marine fatty acids (EPA/DHA) would also have little effect on the point estimate:
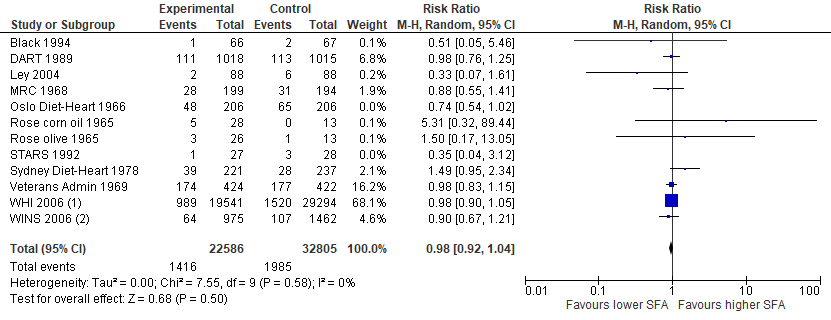 (Image: Cochrane's analysis on total mortality after excluding trials involving increased intakes of marine fatty acids)
(Image: Cochrane's analysis on total mortality after excluding trials involving increased intakes of marine fatty acids)
Some researchers may also object to Cochrane's exclusion/inclusion criteria, which allowed them to exclude the Minnesota Coronary Experiment (6). But including this trial, with or without trials confounded by EPA/DHA, still wouldn't make a big difference:
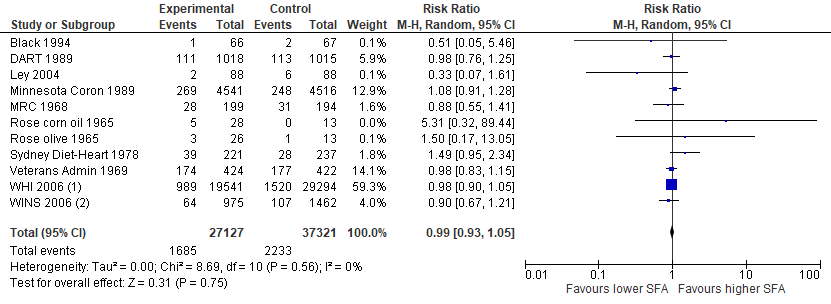 (Image: Cochrane's analysis with the Minnesota Coronary Experiment. Trials confounded by EPA/DHA are excluded)
(Image: Cochrane's analysis with the Minnesota Coronary Experiment. Trials confounded by EPA/DHA are excluded)
These are consistent with Cochrane's 2012 review. In that analysis, Cochrane included the Minnesota Coronary Experiment among other trials not included in their 2020 review. With an even larger sample size involving 4,292 deaths in total, no evidence of a mortality benefit was seen (2).
In short, the lack of effect on mortality is remarkably robust, and all analyses have no significant statistical heterogeneity.
Thus, the most solid conclusion of Cochrane's analysis — the one we can be most certain about — is that "reducing saturated fat intake probably makes little or no difference to all-cause mortality."
Serum Cholesterol and Regressions
Besides the usual meta-analysis, the Cochrane investigators conducted a meta-regression analysis for cardiovascular events and serum cholesterol, claiming:
The data suggested that greater reductions in total serum cholesterol levels reduced CVD events more.
But this result is not robust, as excluding or including one or two trials would remove the association. Furthermore, the causal language is inappropriate, because meta‐regressions are actually observational in nature (7).
As Spineli and Pandis note (8):
The findings of subgroup analysis and meta-regression should be interpreted with caution because of their observational nature. Although patients are randomly allocated to 1 intervention or another within a clinical trial, they are not randomly “allocated” across the trials included in the subgroup and meta-regression analyses. Therefore, subgroup analysis and meta-regression suffer from the same problems and pitfalls as observational studies, such as confounding [and ecological bias].
Nevertheless, since Cochrane did not conduct meta-regressions for mortality outcomes, I wondered what the regressions would look like for total mortality. Therefore, using Cochrane's data, I ran a meta-regression analysis (random effects) and found no significant association between serum cholesterol reductions and mortality.
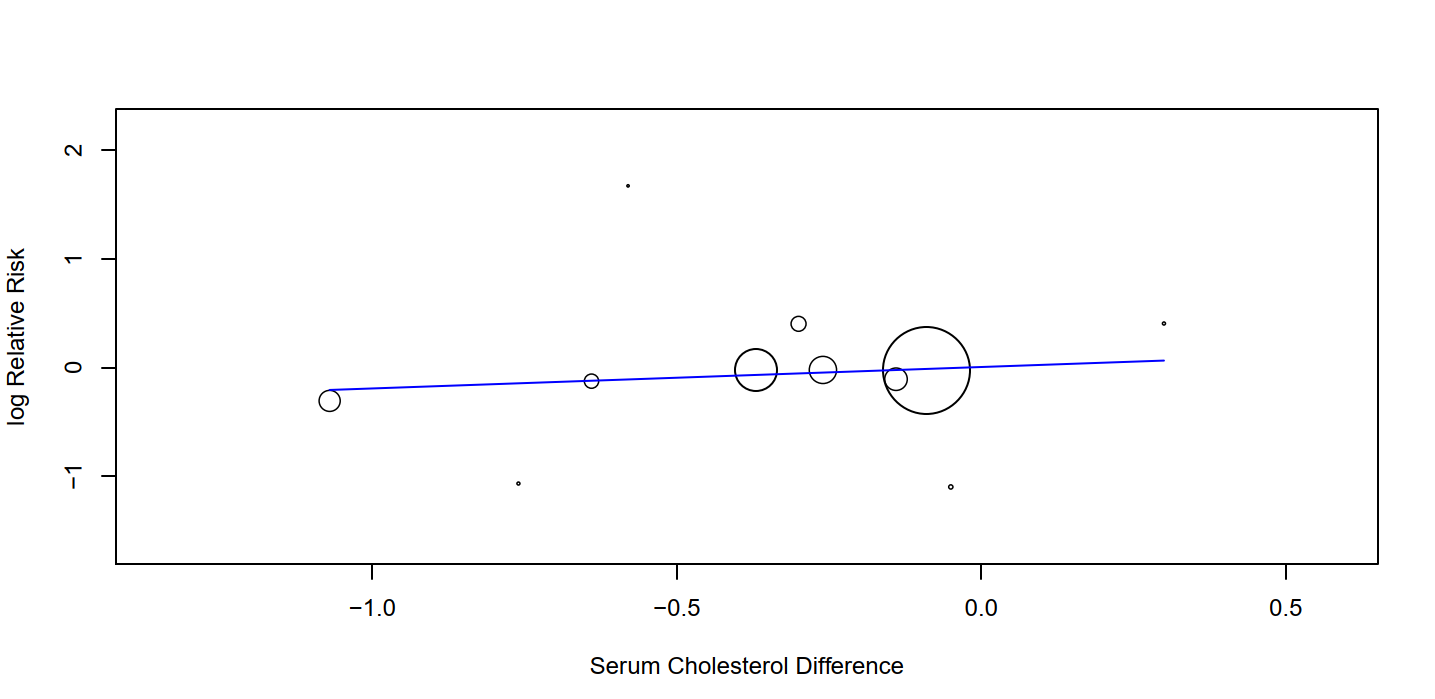 (Image: No significant relation between serum cholesterol and total mortality. P = 0.19)
(Image: No significant relation between serum cholesterol and total mortality. P = 0.19)
There was also no significant relation after excluding trials confounded by marine fatty acids.
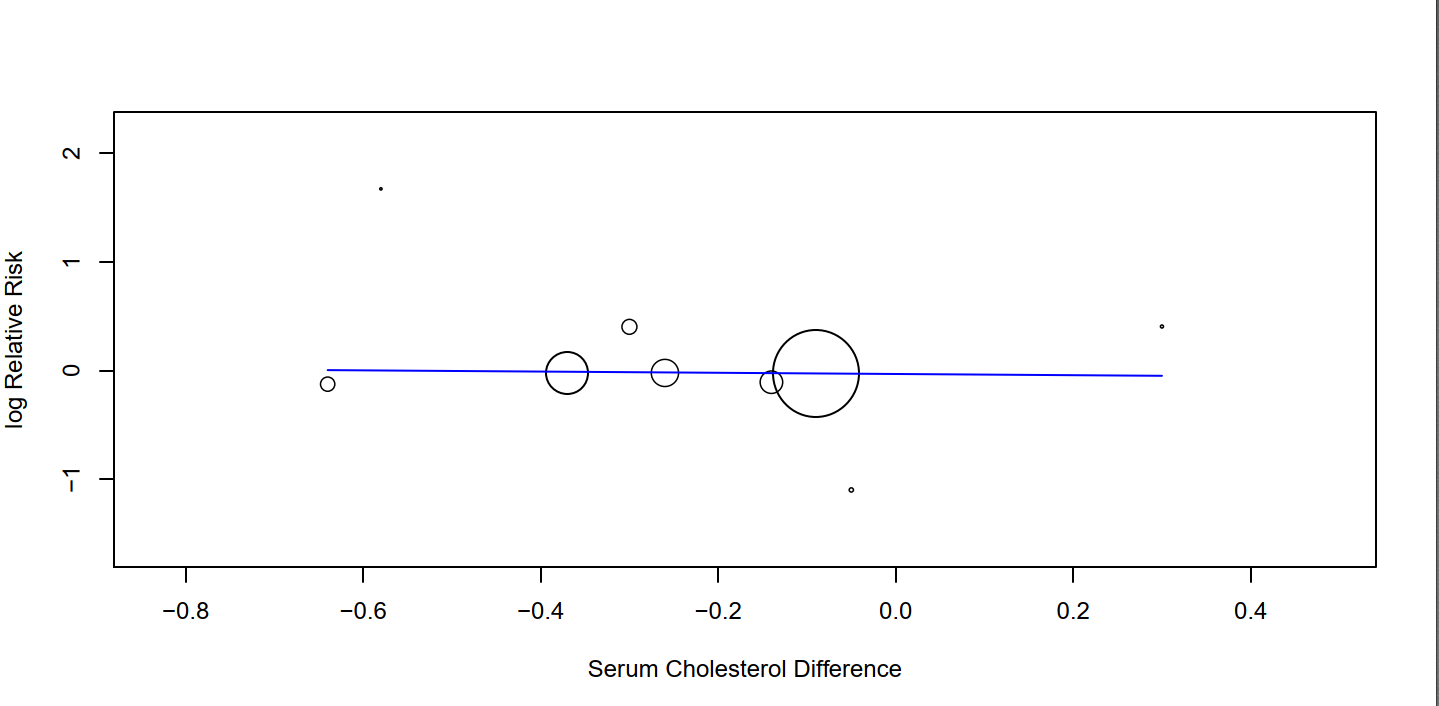 (Image: No significant relation between serum cholesterol and total mortality after exclusion of Oslo and STARS. P = 0.83)
(Image: No significant relation between serum cholesterol and total mortality after exclusion of Oslo and STARS. P = 0.83)
We could additionally look at within-study analyses. For example, observational analyses from the Sydney Diet Heart Study, the Minnesota Coronary Experiment, and the Medical Research Council all showed no association between serum cholesterol and mortality outcomes (6,9,10).
Conclusion
At this point in our context of knowledge, it appears exceedingly unlikely that cutting down on saturated fat would reduce mortality. Therefore, saturated fat remains innocent.
References
1) Hooper, L., Martin, N., Jimoh, O. F., Kirk, C., Foster, E., & Abdelhamid, A. S. (2020). Reduction in saturated fat intake for cardiovascular disease. Cochrane database of systematic reviews, (8). (https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD011737.pub3/epdf/full)
2) Hooper, L., Summerbell, C. D., Thompson, R., Sills, D., Felicia, G. R., Helen, J. M., & Smith, G. D. (2012). Reduced or modified dietary fat for preventing cardiovascular disease. Cochrane Database of Systematic Reviews.
3) Stehbens, W. E. (1993). The lipid hypothesis of atherogenesis. RG Landes.
4) Dayton, S., & Pearce, M. L. (1969). Prevention of coronary heart disease and other complications of atherosclerosis by modified diet. The American journal of medicine, 46(5), 751-762.
5) Jakobsen, J. C., Wetterslev, J., & Gluud, C. (2021). Considerations on the strengths and limitations of using disease-related mortality as an outcome in clinical research. BMJ Evidence-Based Medicine, 26(3), 127-130.
6) Ramsden, C. E., Zamora, D., Majchrzak-Hong, S., Faurot, K. R., Broste, S. K., Frantz, R. P., ... & Hibbeln, J. R. (2016). Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-73). bmj, 353.
8) Spineli, L. M., & Pandis, N. (2020). Problems and pitfalls in subgroup analysis and meta-regression. American journal of orthodontics and dentofacial orthopedics, 158(6), 901-904.
9) Ramsden, C. E., Zamora, D., Leelarthaepin, B., Majchrzak-Hong, S. F., Faurot, K. R., Suchindran, C. M., ... & Hibbeln, J. R. (2013). Use of dietary linoleic acid for secondary prevention of coronary heart disease and death: evaluation of recovered data from the Sydney Diet Heart Study and updated meta-analysis. Bmj, 346, e8707.
10) Morris, J. N. (1968). Controlled trial of soyabean oil in myocardial infarction. Lancet, 2, 693-700.