

The 2019 SARS-CoV-2 pandemic has brought on a multitude of public health measures that have no doubt affected the neurocognitive development of young children, that explained by another recently released study. It is to that degree, masking could be seen as a detriment to the health of young vulnerable, and competent children rather than an advantageous adjuvant in the toolbox of public health mitigation strategies for the reduction of COVID-19.
In this publication 3 things will be examined:
The process a public health intervention like masking children has to go through in order to gain approval for use
How science was ignored relating to the masking of children
The new study from Brown University correlating substantial cognitive decline with masking children
😷 How to properly implement a public masking policy for children
In science, evidence is needed to demonstrate efficacy for proposed public health policy changes. That said, the appropriate way to justify amendments is by using randomized control trials. RCTs serve as the validating factor for all newly proposed interventions.
To begin, randomized control trial (RCT) must be defined. An RCT is a study with a goal of appraising a new interventions effectiveness1. Basically, one group is given a treatment and the other a placebo. After the trial concludes, the results are compared. In other words, did the treatment group benefit more than the other group which received a treatment having no relevant therapeutic value - aka placebo. Moreover, an important part of a RCT is randomization. To explain, randomization is when people are allocated by chance into either a group receiving treatment or placebo. Randomness is an important tool which reduces bias and creates a stronger correlation between the cause an effect of what’s being studied. So after a study has been completed, then what?
The results of many medical RCTs are then uploaded to preprint servers like medRxiv. As it stands, medical studies posted to preprint servers have not formally been peer reviewed or accepted for publication by major medical journals like NEJM, JAMA, The Lancet, Nature Medicine, or PubMed. In other words, the studies have yet to be reviewed by peers within the same field for accuracy2. Regardless, after some period of time, the juvenile publications will soon be ripped apart and analyzed with rigor for approval or denial. If denied, they won’t be posted. If approved, the RCTs will be posted in prestigious journals that will guide the practice of physicians in public and private practice. Said differently, physicians will use the new data to drive new public health policy or guide them in private practice.
All and all, this is the best avenue practitioners have to pilot clinical and public practice. Although, one must keep in mind this avenue isn’t without flaw. So regardless, procession with caution is a necessity especially when handling the health of of others.
🔔 So what does all of this mean?
It is a universally accepted idea that change in public health policy, and practice should be based on RCTs, as they remain the gold standard to best show effectiveness of interventions. So this is how masking children was approved right? WRONG.
👶🏻🧒🏽There is no appropriate science to justify masking children
Considering all the aforementioned information laid out, one would make the educated assumption that our public health officials utilized standard protocols to justify masking all children. Those protocols being sifting through the studies, and implementing interventions from RCTs that showed the best benefit. Unfortunately, that is not the case. To be specific, a couple of points need examining. First, no RCTs were used to justify the sweeping mask policy change for children. Second, large governing health agencies like the CDC, WHO, and UNICEF, are giving conflicting guidance to the public about masking children. The salient facts will be presented below.
Again, just so we’re clear, there are no randomized control trials that exist showing a benefit to masking children. The closest thing that exists is a cluster-randomized controlled trial out of Bangladesh showing an 11.2% reduction in symptomatic seroprevalence from adults using surgical masks, and no benefit from using cloth masks3. That said, adults are not children, so the data in that study couldn’t possibly be reflective of a pediatric population. Moreover, data demonstrating efficacy of an intervention needs to be applied to the cohort it was tested on, so regardless, this study couldn’t be used to justify masking kids. Anyways, the information that did validate masking all children was largely based on flawed observational CDC studies with many confounders correlating case numbers, and outbreaks, in counties with and without school mask requirements45. Regardless, the CDC still gave the green light on masking kids. But that doesn’t discount the confounders of both studies that will be explained below.
The Maricopa study. It claimed the risk of contracting COVID-19 in Maricopa, and Pima counties was 3.5 times higher than schools without mask mandates. The problem, observation time was too short. Results were unfortunately based on a 1 month window. That is bad because 1 month is too little time to draw inference from something that should ideally be looked at for a much longer period of time to prove efficacious. Next, this is an observational study, not a randomized control trial, which means it doesn’t strongly correlate the effect of masking to reduced occurrence of COVID-19. That means, the CDC, a regulatory agency that dictates public health guidance, gave the OK to mask all children in many public, and institutional settings, based on a questionable study that isn’t a gold standard RCT. Moving on, schools in counties with masking requirements had a lot less students. That is bad because comparing schools with lesser enrollees to schools with higher enrollees doesn’t yield accurate results as the final figures would be offset by the size difference of each group. Next, this study does not show the frequency of testing and students who may have been asymptomatic. Simply put, the more testing, the more positive results, the parameters were not defined and that is inappropriate. Essentially, one could test and test and test until a result is obtained. Moreover, asymptomatic cases were not noted, so data does not show the true number of cases. That is improper as the final figure wouldn’t be the result of all cases, only symptomatic ones. Finally, 3.5 x increase in contracting COVID-19 without masking mandates it too substantial compared to the Bangladesh masking study cited earlier in this paper which shows no benefit to cloth masking. All previous confounders, could most certainly justify the final confounding variable which is an inaccurate “3.5 X increase” of spread without school mask mandates.
Now, the next study. It compared all US counties that had a school masking requirement for kids to those that didn’t. The problem, around 83% of places were excluded because their masking policies didn’t match up with the study guidelines. That left a measly 16 +-% to be analyzed. Of course you could understand it would be impossible to extrapolate salient results from only 16% of the population. Notably, the results included positive cases that didn’t attend school ultimately changing the final figures. Those cases shouldn’t have been included as they were not in school and didn’t increase transmission. Finally, total number of cases were not reported, the data was presented in percentages. We need to know the full number of cases because if it was a small figure, again, the data wouldn’t be applicable to the public as a whole.
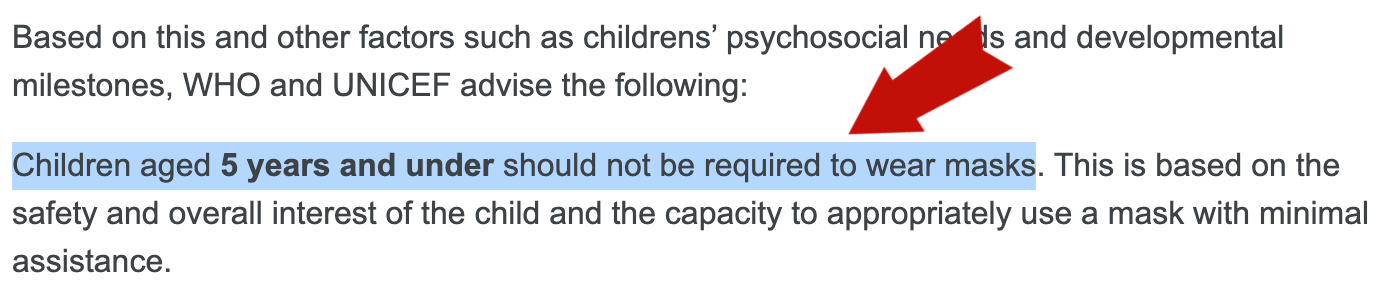
Second, our regulatory public health agencies all seem to have differing opinions on masking children. That is problematic because their guidance needs to be concise and in alliance. For instance, the CDC recommends cloth masking all children 2 and up, while the WHO and UNICEF advise against masking children 5 and under67 (SEE 📸FIG 1&2 below). What’s the public to do if all guidance is conflicting? Furthermore, who regulates the regulators?
📸 FIG. 1

📸 FIG. 2
Here’s the worst part. Now that these mask mandates have been going on for quite sometime, the negatives are surfacing. In light of the consequences to children conferred by masking, public health agencies continue on with the same recommendations.
🔔 So what does all of this mean?
It seems that public health agencies are confused about the correct masking guidance, that evidenced by varying masking recommendations by WHO, CDC, and UNICEF.
📚Brown University study strongly correlates the deleterious effects of COVID-19 rules to poor neurocognitive development in children
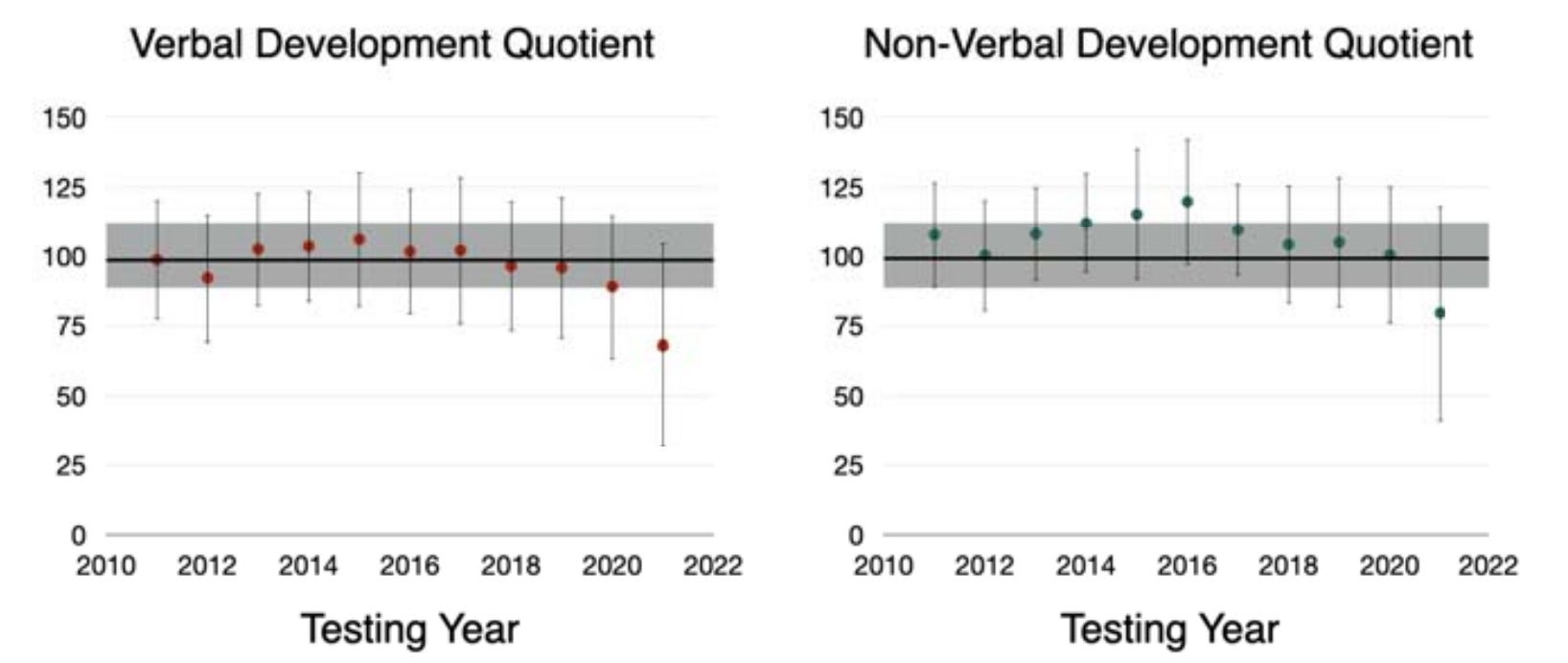
Sadly, a newer study out of Brown University that examined 1,600 children inferred that some SARS-CoV-2 safety measures like masking may impede on children’s neurocognitive development8. Below bullet points will summarize corresponding images:
In 📸 FIG. 3, verbal and non-verbal development quotients substantially decreased beginning 2019 and continued declining through 2021. Verbal development quotients measure the ability of someone to use words, express concepts, and reason. Non-verbal development quotients measure the ability of someone to critically think and problem solve using only visual data received from the environment. That said, the the chart below shows a drop in score of kid’s intelligence since the pandemic began. Masking could have impacted those non-verbal intelligence quotients as they certainly prevent children from reading facial expressions, and appropriately analyzing meaningful non-verbal cues. Verbal communication could be impacted by the fact that masking creates a distortion in peer to peer, and child to teacher communication leaving children unable to fully comprehend what same aged companions, or even teachers are trying to elucidate. All of that the authors suggest, could be leaving these kids at a deficit. Masking isn’t the only thing to blame, however the data suggests could be playing a huge role
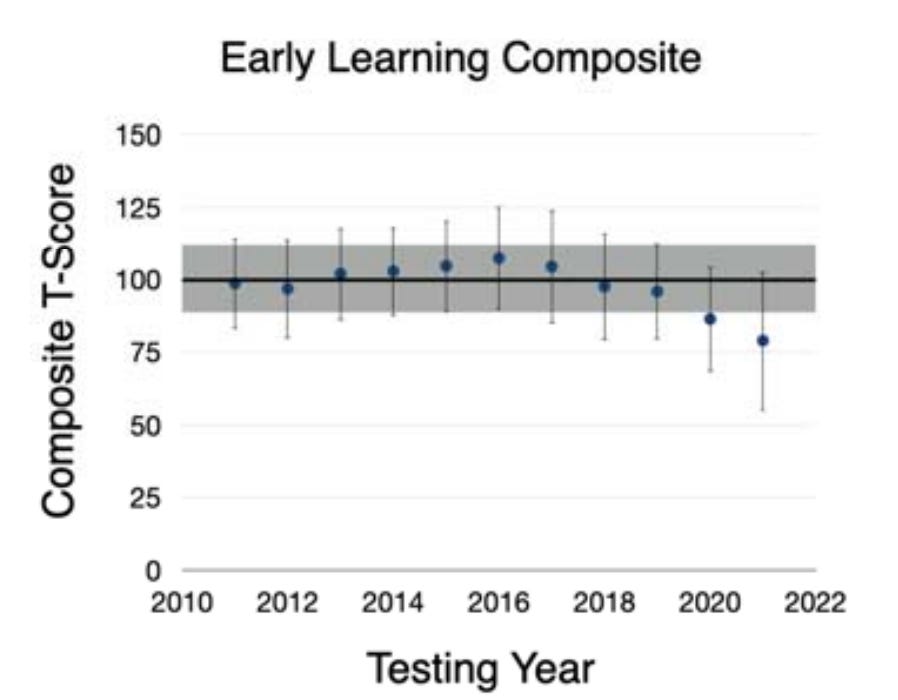
Finally, 📸 FIG. 4 shows a 23% reduction in early learning composite scores since the pandemic began. This measures the efficiency of a child’s receptive + expressive language, fine motor skills, and visual reception. Again the authors infer such results could be from masking creating a barrier to development.
If that’s not enough for you, here are more studies showing the damage done to kids by masking:
🔔 So what does all of this mean?
It seems data is mounting to show masking children could be causing some serious problems. That said, public health official need to consider amending current masking policies for our most vulnerable.
📸 FIG. 3
📸 FIG. 4
🤔Knowing all that should we keep masking kids?
You see, if the scientific process was followed, health agencies didn’t provide conflicting guidance about masking kids, and data wasn’t surfacing on the detrimental effects from masking children, i’d say it would be wise to continue on with the plan. Unfortunately, the anthesis is happening. That said, public health policy needs to change because continuing on with interventions that are now showing to be more harmful than helpful, will reduce public confidence in the medical system, and most importantly harm kids. After reading everything above, how do you feel about about masking children?
LETS CONNECT:
RESEARCH:
1 https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC6235704/
2 https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC4975196/
3 https://www.poverty-action.org/publication/impact-community-masking-covid-19-cluster-randomized-trial-bangladesh
4 https://www.cdc.gov/mmwr/volumes/70/wr/mm7039e1.htm
5 https://www.cdc.gov/mmwr/volumes/70/wr/mm7039e3.htm?scid=mm7039e3w#contribAff
6 https://www.cdc.gov/coronavirus/2019-ncov/community/schools-childcare/k-12-guidance.html#:~:text=Consistent%20and%20Correct%20Mask%20Use&text=Indoors%3A%20CDC%20recommends%20indoor%20masking,to%20wear%20masks%20when%20outdoors.
7 https://www.who.int/news-room/questions-and-answers/item/q-a-children-and-masks-related-to-covid-19
8 https://www.medrxiv.org/content/10.1101/2021.08.10.21261846v1.full.pdf